NYACP Board Review Question of the Week
![]()
Every other Tuesday, NYACP members are sent a Board Review Question from ACP's MKSAP 18 to test professional knowledge and help prepare for the exam. Participant totals and answer percentages are distributed on the first Thursday of the month in IM Connected, the Chapter's eNewsletter, and are also published on this page.
If you are interested in receiving these questions bi-weekly, join us as a member!
If you are a member who needs to receive the questions and newsletter via email, let us know!
March 24th, 2026
MKSAP 19 Cardiovascular Medicine, Question 52
An 84-year-old man is evaluated before hospital discharge following an exacerbation of heart failure. He has an implantable cardioverter-defibrillator. Medications are lisinopril, furosemide, carvedilol, and spironolactone. During hospitalization, the patient received intravenous furosemide at a dosage twice that of his home oral dosage.
On physical examination, vital signs are normal. BMI is 28. Central venous pressure is not elevated. There is no S3, and there are no pulmonary crackles.
Serum creatinine level has returned to the baseline level, and electrolytes are normal. Echocardiogram from this hospitalization shows ejection fraction of 25% with left ventricular end- diastolic dimension of 72 mm.
Which of the following is most likely to prevent early hospital readmission in this patient?
A. Echocardiography in 3 months
B. Follow-up office visit in 30 days
C. Follow-up telephone call in 2 days
D. Decrease in furosemide to original home dosage
Responses Received from Members (705 Responses):
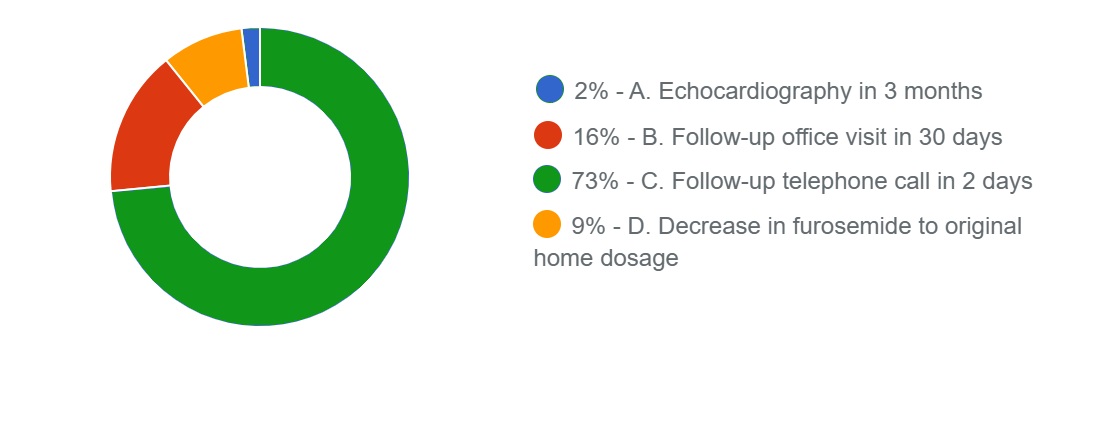
The Correct Answer is: C. Follow-up telephone call in 2 days
Educational Objective: Prevent heart failure readmission with early follow-up.
A telephone call within 2 to 3 days (Option C) is recommended to prevent this patient's early readmission to the hospital. The 2019 American College of Cardiology expert consensus decision pathway for patients hospitalized with heart failure notes that up to 25% of patients are readmitted with heart failure within 30 days of the index hospitalization. Two key elements are associated with a successful transition from hospital to home: a follow-up phone call within 2 to 3 days of discharge and an office visit within 7 to 14 days of hospital discharge. The purpose of the follow-up phone call is to address signs of congestion, provide education and review adherence to the medication regimen, and confirm follow-up appointments and adequate transportation. The expert consensus decision pathway recommends a standardized approach to the follow-up telephone call, including use of a checklist to help organize the call.
For patients with an initial diagnosis of heart failure, it is appropriate to repeat echocardiography in 3 months (Option A) to assess the effect of medical therapy on ejection fraction and need for an implantable cardioverter-defibrillator (ICD). Echocardiography was performed in this patient in the hospital, and for a patient with known low ejection fraction and an ICD, there is no reason for echocardiography so soon unless there is a clinical change.
The first postdischarge appointment focuses on changes in clinical status, patient education, medication review and adjustment of dosages, and identification and correction of issues that might lead to worsening of heart failure and readmission. The recommended timing of the first follow-up visit is within 7 to 10 days of hospital discharge; 30 days (Option B) is too late.
Inadequate diuretic dosage is a common cause of heart failure readmissions. This patient required an increased furosemide dosage to achieve adequate diuresis. This suggests that the previous home diuretic dosage was inadequate, and an increase of at least double that dosage should be considered.
Restarting the previous home dosage (Option D) might be considered for a patient who did not adhere to the medication regimen before hospitalization.
Key Point
- Two key elements are associated with a successful transition to home following hospitalization for heart failure: a follow-up phone call within 2 to 3 days of discharge and an office visit within 7 to 14 days of hospital discharge.
Bibliography
Hollenberg SM, Warner Stevenson L, Ahmad T, et al. 2019 ACC expert consensus decision pathway on risk assessment, management, and clinical trajectory of patients hospitalized with heart failure: a report of the American College of Cardiology Solution Set Oversight Committee. J Am Coll Cardiol.
2019;74:1966-2011. PMID: 31526538 doi:10.1016/j.jacc.2019.08.001
Multiple-choice questions reprinted with permission from the American College of Physicians.
MKSAP 19. © Copyright 2021 American College of Physicians.
ACP MKSAP. © Copyright 2025 American College of Physicians. All Rights Reserved All Rights Reserved.
March 10th, 2026
MKSAP 19 Endocrinology & Metabolism, Question 69
A 23-year-old woman is evaluated for persistent hirsutism related to polycystic ovary syndrome (PCOS). She presented for evaluation 6 months ago with irregular menstrual cycles, coarse facial and body hair, and obesity. Diabetes screening was normal. Combined oral contraceptive therapy was prescribed along with weight loss. She has been adherent to this treatment and now has monthly withdrawal vaginal bleeding; she also has lost 4.5 kg (10.0 lb). She has had some improvement in hair growth but is not completely satisfied.
Vital signs are normal. BMI is 30. She has dark, coarse hair over her chin, upper lip, chest, back, pubic area, arms, and legs. No evidence of virilism is noted.
Which of the following is the most appropriate next step?
- Add metformin
- Add spironolactone
- Obtain adrenal CT
- Obtain pelvic ultrasonography
Responses Received from Members (663 Responses):
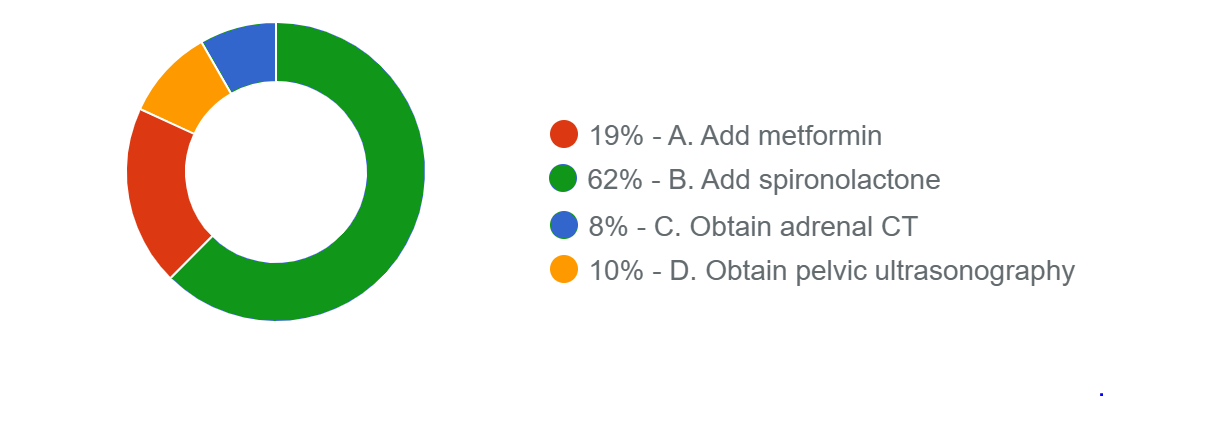
The Correct Answer is: B. Add spironolactone
Educational Objective: Treat hirsutism in a patient with polycystic ovary syndrome.
The most appropriate next step is to add spironolactone (Option B). Polycystic ovary syndrome (PCOS) is a disorder characterized by hyperandrogenism and ovulatory dysfunction. PCOS affects 6% to 10% of women and is the most common cause of anovulatory infertility in women. It is associated with rapid gonadotropin-releasing hormone pulses, an excess of luteinizing hormone, and insufficient follicle-stimulating hormone secretion, resulting in excessive ovarian androgen production and ovulatory dysfunction. PCOS is accompanied by insulin resistance. Elevated insulin levels in PCOS further enhance ovarian and adrenal androgen production, as well as increase bioavailability of androgens related to a reduction in sex hormone-binding globulin. PCOS is associated with increased incidence of metabolic syndrome, prediabetes, type 2 diabetes mellitus, hypercholesterolemia, and obesity. This patient with PCOS has evidence of ongoing hirsutism (i.e., dark coarse hair on the face, chest, back, arms/legs) and acne despite 6 months of oral contraceptive therapy. The next step is to add an antiandrogen agent to oral contraceptive therapy. Spironolactone is the most commonly used antiandrogen agent and is generally safe and well tolerated. Potential adverse effects include hyperkalemia (rare in patients with normal renal function), gastrointestinal discomfort, and irregular menstrual bleeding. In women prescribed spironolactone, concomitant contraception is mandatory because of teratogenesis in male fetuses.
Metformin (Option A) reduces hyperinsulinemia and androgen levels but has minimal impact on hirsutism and ovulation. Metformin is indicated when impaired glucose tolerance, prediabetes, or type 2 diabetes does not respond adequately to lifestyle modification. This patient has a negative screening test for diabetes and thus has no indication for metformin.
Rapid onset of hirsutism or virilization (voice deepening, clitoromegaly, male pattern baldness, severe acne) occurs only in severe hyperandrogenism and raises concern for ovarian hyperthecosis or an androgen-producing ovarian or adrenal tumor. This patient does not have features of virilization or rapid-onset hirsutism. Because an adrenal or ovarian tumor is unlikely, an adrenal CT (Option C) or pelvic ultrasonography (Option D) is not indicated.
Key Point
- In women with polycystic ovary syndrome and hirsutism, an antiandrogen agent such as spironolactone should be added after 6 months if cosmesis is suboptimal with oral contraceptive agents alone.
- Antiandrogen agents may adversely affect development of the male fetus and therefore should not be used in the treatment for polycystic ovary syndrome without concomitant contraception.
Bibliography
McCartney CR, Marshall JC. Clinical practice. Polycystic ovary syndrome. N Engl J Med. 2016;375:54-
64. PMID: 27406348 doi:10.1056/NEJMcp1514916
Multiple-choice questions reprinted with permission from the American College of Physicians.
MKSAP 19. © Copyright 2021 American College of Physicians.
ACP MKSAP. © Copyright 2025 American College of Physicians. All Rights Reserved All Rights Reserved.